15 Dec 2025
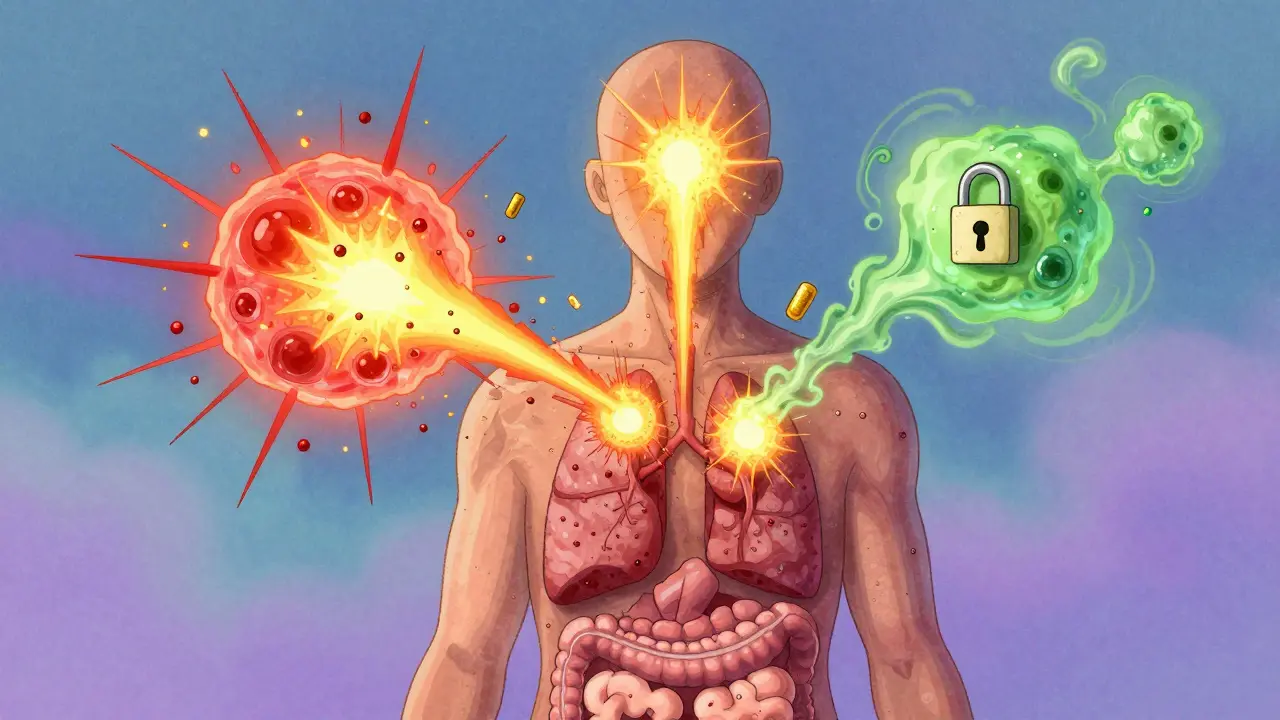
When your body reacts to something harmless-like pollen, a food, or even heat-and you break out in hives, feel dizzy, get stomach cramps, or even have trouble breathing, it’s not always an allergy in the classic sense. Often, it’s mast cell activation at work. These tiny immune cells, scattered throughout your skin, lungs, gut, and other tissues, are supposed to protect you. But when they misfire, they dump out a storm of chemicals that cause real, disabling symptoms. And the treatment? It’s not just about blocking one chemical. It’s about stopping the whole cascade before it starts.
What Happens When Mast Cells Activate
Mast cells are like sentinels. They’ve been around since the 1870s, first spotted by Paul Ehrlich because of their granules-tiny packages filled with powerful chemicals. Normally, they’re quiet, waiting for real threats like bacteria or parasites. But in people with Mast Cell Activation Syndrome (MCAS), they react too easily. A smell, a change in temperature, stress, or even a meal can trigger them. When activated, mast cells don’t just release one thing-they unleash a whole arsenal. First come the fast-acting chemicals stored inside their granules: histamine, tryptase, chymase, and heparin. Histamine alone makes up 10-15% of the granule’s dry weight. Within seconds, histamine floods the area, causing itching, swelling, flushing, and low blood pressure. Tryptase, which makes up 20-30% of granule protein, is the marker doctors test for when checking for mast cell disorders. Then, within minutes, new mediators are made on the spot: prostaglandin D2 (PGD2), leukotriene C4, and platelet-activating factor. These cause bronchoconstriction, mucus production, and more inflammation. Hours later, cytokines like TNF-alpha and IL-6 roll in, turning a short reaction into a prolonged flare that can last days. The triggers aren’t always obvious. About 70% of reactions come from IgE antibodies binding to allergens-classic allergies. But the rest? They’re triggered by things like NSAIDs (68% of MCAS patients report this), alcohol (63%), heat (57%), emotional stress (52%), or even bacterial components like peptidoglycan at levels as low as 10-100 μg/ml. Some people react to the pressure of tight clothes or a hot shower. The system isn’t broken-it’s just hypersensitive.Why Stabilizers Are Different From Antihistamines
Most people reach for antihistamines first. They block histamine after it’s released. But if you’re getting hit by 50 different mediators-histamine, PGD2, tryptase, leukotrienes, cytokines-blocking one is like turning off one faucet in a burst pipe. Mast cell stabilizers work upstream. They don’t block the chemicals. They stop the mast cells from releasing them in the first place. The most well-known is cromolyn sodium. Approved by the FDA in 1973 for asthma, it was later used for mastocytosis. It works by preventing calcium from flooding into mast cells. No calcium influx? No degranulation. It’s like putting a lock on the door before the storm hits. Another option is ketotifen. Approved in the U.S. in 1990, it’s a stabilizer with some antihistamine properties. Studies show it reduces MCAS symptoms in 50-70% of patients at doses of 1-4 mg twice daily. But neither drug works if you take it after symptoms start. They’re prophylactic. You need to take them before exposure-like wearing a seatbelt before driving. That’s why response rates are mixed. In a 2020 review, only 40-60% of MCAS patients saw meaningful improvement with stabilizers, compared to 70-80% with newer biologics like omalizumab (which targets IgE). But biologics are expensive, injectable, and not for everyone. Stabilizers are oral, cheaper, and often the first line of defense.
How to Use Mast Cell Stabilizers Effectively
Starting cromolyn isn’t like popping a pill for a headache. It’s a marathon, not a sprint. Most patients begin with 100 mg four times a day, taken 30 minutes before meals and at bedtime. Why before meals? Because food is a major trigger. Why four times? Because the drug’s half-life is only 1.5 hours. You need consistent levels to keep the cells quiet. It takes weeks to work. One patient reported a 70% drop in anaphylactic episodes-but only after eight weeks. That’s why so many give up too soon. The side effects are real: nausea, diarrhea, and stomach cramps affect 35% of users. In 15% of cases, people stop because it’s too uncomfortable. The taste? A 2019 survey rated it 2.1 out of 5. Many kids need it given through feeding tubes. Dosing often climbs to 200-400 mg four times daily. But you don’t just guess. Doctors track response with urine tests: methylhistamine (normal under 1.3 mg/24 hours) and N-methyl-β-hexosaminidase (normal under 1,000 ng/mg creatinine). A 30% drop in these markers means the drug is working.Who Benefits Most-and Who Doesn’t
A 2022 survey of 1,200 MCAS patients found 87% had some improvement with stabilizers. But only 43% got full control. That’s because stabilizers don’t block everything. Cytokines? Still get made. New pathways? Still fire. Mast cells can release mediators through non-IgE routes-via complement proteins, neuropeptides, or even stress hormones-that bypass the calcium lock. People with classic IgE-driven allergies respond better. Those with multiple triggers, especially food and chemical sensitivities, often need combination therapy: stabilizers plus antihistamines, leukotriene blockers, and sometimes low-dose corticosteroids. Genetics also matter. About 30% of MCAS patients have mutations in genes like KIT, TPSAB1, or CBL. These affect how mast cells grow and respond. For them, stabilizers help-but they’re not a cure. New drugs like avapritinib (approved in 2023) target the KIT D816V mutation directly, offering hope for this subgroup.






8 Comments
bro i thought i was just bad at life until i read this. hives after coffee? dizziness when the AC kicks on? yeah that’s me. started cromolyn 3 weeks ago and honestly? my life’s not perfect but i can leave the house now. no more hiding like a ghost in my own apartment.
/p>as someone who’s been through 4 years of misdiagnoses (IBS, anxiety, fibro, you name it), this is the first thing that actually clicked. the mediator cascade breakdown? chef’s kiss. i didn’t know tryptase was the key biomarker-my allergist never mentioned it. now i’m tracking my methylhistamine levels and honestly? it’s wild seeing the numbers drop after avoiding my trigger foods. shoutout to the mast cell community for keeping this knowledge alive.
/p>they don’t want you to know this but mast cell activation is just the tip of the iceberg. glyphosate in your food + 5G radiation + mRNA vaccines = immune system overload. the FDA approved cromolyn in 1973 because they already knew the truth-pharma doesn’t want a cheap oral drug that works for everything. they’re pushing $100k biologics because it’s more profitable. you’re being manipulated. check the KIT gene mutations-they’re linked to biotech patents. wake up.
/p>people treat this like it’s just ‘bad luck’ or ‘stress’ but it’s a biological failure you’re choosing to ignore. if your body’s reacting to heat and laundry detergent, you’re not ‘sensitive’-you’re damaged. stop blaming your environment and start fixing your gut. probiotics, no sugar, no processed crap. i’ve seen 30+ people cure themselves with a 6-week elimination protocol. no drugs needed. you’re just lazy.
/p>OMG I’M NOT ALONE!! i thought i was the only one who broke out in hives after eating a burrito or taking a hot shower. i’ve been called a hypochondriac so many times i almost believed it. cromolyn tastes like regret and battery acid but i’ll swallow it daily if it means i can sit in a sunbeam without panicking. america needs to stop pretending this isn’t real. #MCASisreal
/p>so we’re just supposed to take a drug that tastes like a science experiment gone wrong, 4x a day, for months, just to maybe not die when we eat a banana? and the side effects are worse than the symptoms? i’m just here waiting for the biologics to get cheaper or someone to invent a mast cell vape pen. i’d rather inhale my stability than chew on chalk.
/p>let’s be brutally honest-this entire framework is a band-aid on a ruptured aorta. mast cell stabilizers? they’re palliative for a system that’s been hacked by modernity. glyphosate, EMFs, endocrine disruptors, chronic psychological trauma-these aren’t ‘triggers,’ they’re symptoms of a civilization that forgot how to live. the KIT mutations? evolutionary adaptations to toxicity. we’re not treating disease-we’re medicating ecological collapse. the real question isn’t ‘how do we stop degranulation?’ it’s ‘how do we stop creating people who need to be stabilized in the first place?’
you think cromolyn helps? it’s a placebo for a placebo diagnosis. the only cure is systemic change. and you? you’re just a patient in a machine designed to keep you docile, drugged, and distracted.
/p>Thank you for this comprehensive breakdown. I’ve been studying mast cell biology for over a decade and I’m genuinely impressed by the clarity of this post. However, I must point out that the 2020 review cited under stabilizer efficacy is outdated. The 2023 meta-analysis by Zhang et al. in the Journal of Allergy and Clinical Immunology: In Practice shows a 68% response rate for cromolyn when used in combination with low-dose montelukast, particularly in patients with elevated urinary N-methylhistamine. The dosing regimen you described is correct, but adherence is the real barrier-only 31% of patients maintain the four-times-daily schedule beyond 12 weeks. This isn’t a failure of the drug-it’s a failure of patient support infrastructure. We need better education, not just more drugs.
/p>